Treatment for Gamekeeper's and Skier's Thumb
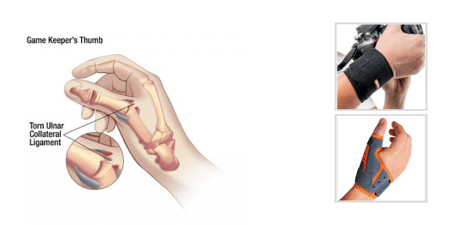
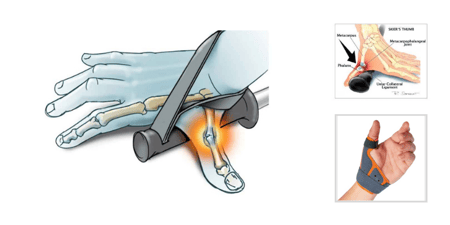
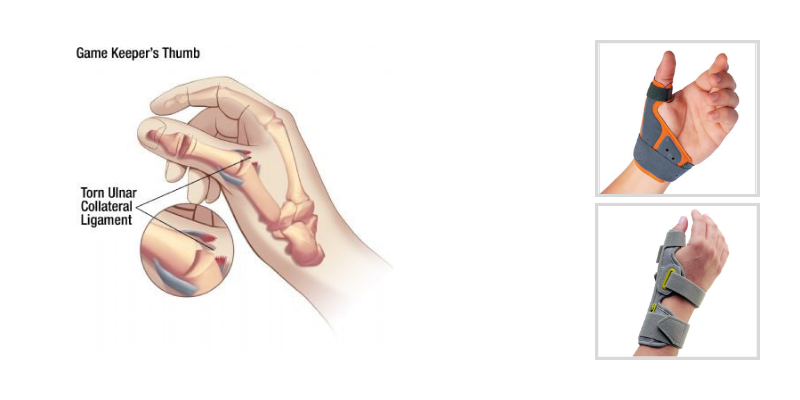
Injuries to the thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) are common following trauma or repetitive stress and can significantly impact pinch strength, grip stability, and hand function. The thumb MP joint is stabilized by collateral ligaments on both the radial and ulnar sides of the joint. The UCL plays a critical role in maintaining lateral pinch stability and is particularly vulnerable when a radial deviation and hyperextension force is applied to the thumb MP joint.
An acute injury is commonly referred to as Skier’s Thumb, occurring when the thumb is forcefully abducted and hyperextended—often during a fall while holding a ski pole. In contrast, Gamekeeper’s Thumb describes a chronic overuse injury caused by repetitive grasping, pinching, or twisting activities that gradually stretch or tear the UCL over time.
Evaluation of Thumb UCL Injuries
A suspected UCL injury should be evaluated for instability and ligament laxity. Stress testing is typically performed by applying an ulnar-directed force to the proximal phalanx while stabilizing the metacarpal radially. The thumb MP joint is positioned in approximately 30 degrees of flexion to minimize support from the volar plate and isolate the ligament.
It has been suggested that the following may indicate a complete rupture of the UCL:
-
30–40 degrees of laxity, or
-
Laxity exceeding 15 degrees compared to the contralateral thumb
Because baseline thumb MP joint laxity varies among individuals, bilateral comparison is essential during assessment.
Diagnostic imaging may also assist with evaluation, including:
-
Radiographs to assess for avulsion fractures
-
MRI for soft tissue integrity
-
Ultrasound imaging for dynamic ligament assessment
Treatment Options for Gamekeeper’s and Skier’s Thumb
| Type | Description | Treatment |
| Partial or minimally displaced UCL tear or UCL Sprain | Pain with palpation, no obvious laxity with stress testing or laxity comparable to the non-involved thumb | Full time use of an orthosis that prevents stress to the thumb MP joint for 4-6 weeks to allow healing and scarring of the UCL (Many physicians prefer a forearm based orthosis initially to ensure no stress is applied to the joint) |
| UCL Tear | A complete tear of the UCL can be identified with obvious laxity during stress testing (see above) or with imaging of the soft tissue | Usually requires surgical repair of the ligament or reconstruction of a chronic tear (Less than 3 mm of displacement of the ligament has been found to respond to conservative immobilization) |
| UCL Tear with Avulsion Fracture | Injury to the UCL with avulsion fracture of the thumb proximal phalanx where the UCL inserts onto the bone | If the fracture is stable, casting or full time orthosis use protecting the thumb MP joint is recommended. When the fracture is not stable, surgery is needed for fracture stabilization. |
| UCL Tear with Stener’s Lesion | The adductor aponeurosis is interposed between the distally avulsed UCL and its attachment on the base of the proximal phalanx, which prevents healing (and may be palpated) | Surgery is required for repair of the ligament |
Rehabilitation and Orthotic Management
Following surgical repair or conservative treatment, immobilization of the thumb MP joint is typically recommended to protect healing tissues and reduce stress across the UCL. As healing progresses, transition to removable orthoses can support gradual return to functional activities while maintaining stability.
There are several orthotic options that may assist during the rehabilitation process and later healing stages, including:
These orthoses are designed to help protect the thumb MP joint while allowing functional hand use during
 |
 |
 |
| 3pp® ThumSaver™ MP | Fix Comfort Thumb Brace | 3pp® Ez FIT Thumb Spica Splint |