Even though Spring is officially around the corner, many parts of the country are still experiencing winter storms. Snowy and icy conditions often lead to wrist fractures caused by a fall on an outstretched hand (FOOSH). There are a few tricks to the trade to effectively rehab these mishaps.
The 3pp Wrist Wrap NP and the 3pp Wrist POP are examples of supports that can help individuals recover from wrist pain related to strains and sprains, post-operative, or post casting after a FOOSH.
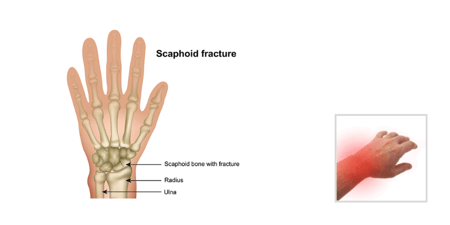
Addressing range of motion after a distal radius fracture
Once the cast or external fixators are removed, the work of restoring finger, wrist and forearm motion starts in earnest. Composite finger flexion, wrist extension, and supination are motions important to functional use of the hand, and these motions are commonly limited after a wrist fracture.
- Intrinsic tightness (preventing a hook fist) and weakness or stiffness in wrist extension can result in limited finger flexion following a distal radius fracture.
- When wrist extension is performed with the fingers straight or just the MCP joints extended, the extensor digitorum communis (EDC) or long wrist extensor tries to pull the wrist back. Performing wrist extension with the fingers in a full fist is a good exercise is important to retrain and strengthen the short wrist extensors.
- Step-by-step repetition of the normal mechanics of making a fist is key to restoring full motion. Exercises should be done slowly to assure each component motion is achieved fully and is maintained as the next motion is added.
- Start in a position of full finger and wrist extension as possible.
- With the wrist and MCP’s in extension, move the fingers into the hook position (distal and proximal interphalangeal flexion). Manually blocking the MCP’s or using a blocking splint may be necessary at the outset to restrict MCP flexion.
- Gradually add MCP flexion making certain the wrist stays extended and the IP’s maintain full flexion.
- Reverse the pattern: extend the MCP’s; straighten the IP’s and keep the wrist extended.
The importance of therapy working to restore forearm supination after a wrist fracture is best appreciated by the person who has lost or restricted supination.
- It is often a challenge to avoid substituting shoulder motion to compensate for loss of supination. When performing supination exercises, the elbow must be bent and tucked at the side of the body to prevent compensation. Use a strap or exercise band around the body and upper arm to act as a restraint to shoulder motion.
- A suggested exercise to help the patient do supination exercises is the “towel twist”.
- Secure one end of a hand or kitchen towel in a closed door.
- Standing in front of the door, holding the other end and, using both hands, twist the towel until it is tight.
- Standing with the arm bent and firmly pressed against the body, grasp the towel with the forearm pronated (palm down) and the wrist straight. Turn into supination and back into pronation for several repetitions. This exercise encourages full fisting and supination and gives a visual cue to the degree of supination achieved. Over time, the towel can be twisted tighter for resistance and strengthening.
A distal radius fracture can have significant functional ramifications and a well organized and communicated therapy program is essential to an optimal outcome.
3pp® Wrist Wrap NP

3pp® Wrist POP™ Splint


Blog References: For more info on this topic, click to see the references for this blog post.