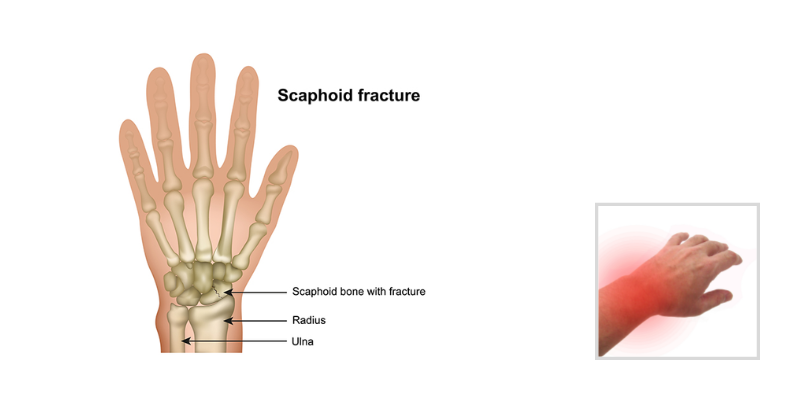
Scaphoid fractures most often occur in males between the ages of 15 to 30 years old and usually are sustained with wrist hyperextension and radial deviation as a consequence of a fall onto an outstretched hand. Individuals with a scaphoid fracture often present with pain, swelling, decreased range of motion, and tenderness in the anatomic snuffbox.
Treatment Options of a Scaphoid Fracture
Stable, non-displaced fractures at the waist (mid scaphoid) or distal scaphoid (top of the bone) are often treated with thumbspica casting for 8-12 weeks. Fractures in the proximal portion, (closer to the wrist) where the scaphoid has a poor blood supply, can result in complicated or prolonged healing. These proximal fractures frequently require surgery for either a pin or screw fixation to allow healing. A Scaphoid nonunion (unhealed older fracture) is treated surgically with a bone graft and hardware fixation, followed by immobilization to allow healing.
Evaluation and Rehabilitation Following a Scaphoid Fracture
The therapy evaluation for an individual who has had a scaphoid fracture should include range of motion and strength assessment as permitted by the treating physician, measurement for edema, pain rating, and completion of a patient-rated functional outcome measure to assist with identifying functional concerns. Due to a possible need for prolonged immobilization, proprioception can be impacted. Proprioception may be assessed with joint position sense testing (where a wrist position needs to be replicated after placement into the position by the assessor).
When an individual is referred to therapy while still immobilized in a cast or non-removable orthosis, there are a few important things to consider. Range of motion at the non-involved joints of the digits, forearm, elbow and even shoulder should be evaluated and addressed as appropriate. The patient should be using the involved extremity for light functional tasks and edema management can be addressed as needed (i.e. Coban wrapping of the digits, overhead pumping).
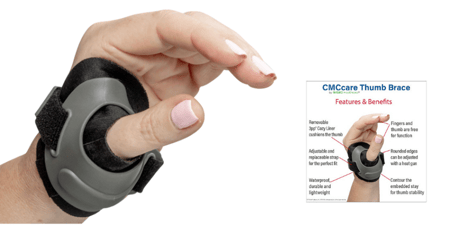
Once there is clinical healing on radiographs, the immobilization phase is usually over. Typically a Thumb Spica orthosis is then used for comfort and protection. The 3pp Ez FIT Thumb Spica Splint is ideal for protection of the wrist and thumb following a scaphoid fracture.

A well-directed program of wrist and thumb range of motion can commence. It is important the patient is educated in the need for follow through with a documented exercise program and the knowledge that return to full range of motion and activities will take time. The therapeutic program can be progressed as appropriate to include passive stretching and eventually strengthening exercises. Functional outcomes after a scaphoid are good, so therapy goals to return to functional motion and strength and everyday functional tasks are appropriate.

Blog References: For more information on this topic, click to see the references for this blog post