

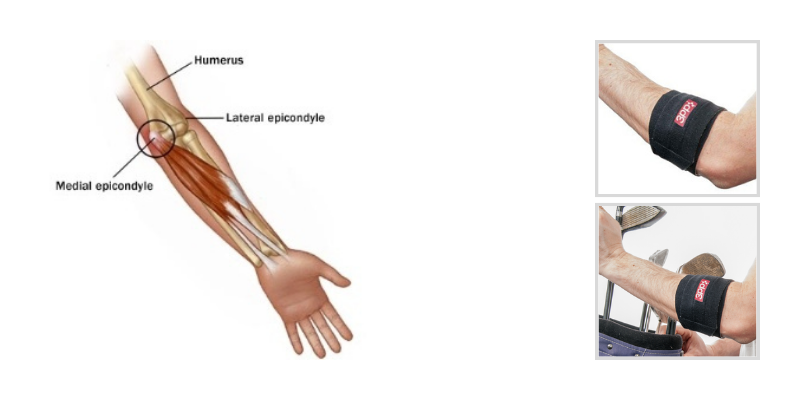
Medial epicondylitis or golfer's elbow as it is commonly termed, is characterized by pain at or around the boney prominence at the medial aspect of the elbow where the wrist flexors and one of the forearm pronators (pronator teres) originate. This diagnosis is associated with degenerative changes of the musculotendinous origins at the medial elbow and most often involves the pronator teres, flexor carpi radialis or palmaris longus. These pathologic changes are primarily the result of overuse of the originating muscles which causes microtears and a subsequent incomplete reparative process of the soft tissue.
Occurrence of Medial Epicondylitis
The diagnosis of medial epicondylitis is more common in women than men and occurs most often between ages 40-60. The prevalence of medial epicondylitis is significantly lower at between 0.3-1.1% than that of lateral epicondylitis (Tennis Elbow) at 1.0-3.0% of the general population. According to research study, forceful activities, high force combined with high repetition or awkward postures are associated with epicondylitis. Despite the layman’s term of golfer’s elbow and the fact that the mechanics of a golf swing may cause symptoms of this diagnosis, it also occurs commonly with throwing athletes and individuals who use large hand tools such as chainsaws and axes.
Diagnosis of Medial Epicondylitis
A diagnosis of medial epicondylitis is often made by a physician based on clinical presentation. There is often pain with palpation at the flexor pronator origin at the medial epicondyle or pain with a stretch to the flexor pronators (forearm supination with wrist and elbow extension). Resistance to the wrist flexors and/or pronator should also elicit pain. An MRI can be used to confirm diagnosis or evaluate the status of the tendons, but is not routinely used.
Treatment of Medial Epicondylitis
Conservative treatment for medial epicondylitis involves anti-inflammatories, exercises, modalities, bracing and strapping, and activity modification. Individuals should avoid aggravating activities and those that load the wrist flexors and pronators. Wrist neutral posture should be encouraged. Wrist braces and forearm straps are meant to decrease the stress to and the overuse of the wrist flexors and forearm pronator. Modalities, such as ice, heat, ultrasound, and electrical stimulation, are used to decrease edema and increase soft tissue elasticity and may therefore decrease pain. Exercises include gentle stretches and eccentric strengthening to assist healing. If conservative treatments fail, surgery for debridement and or repair of the involved tendons may be warranted.
The 3pp Elbow POP Splint may be appropriate to address symptoms from medial epicondylitis. The Elbow POP’s adjustable point of pressure (POP) can be used for the musculotendinous origin at the medial elbow to decrease tension and pull on the irritated soft tissues. The design allows pressure according to individualized symptoms without application of circumferential pressure. There is also a designed sleeve for fashion and function (covering the strap so hook straps do not get caught on clothing).
3pp® Elbow POP™ Splint
 For more information on the 3pp Elbow POP Splint click on the button below
For more information on the 3pp Elbow POP Splint click on the button below


Blog References: For more information on this topic, click to see the references for this blog post.

