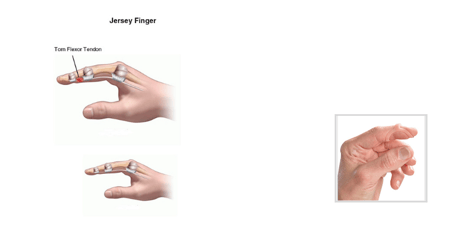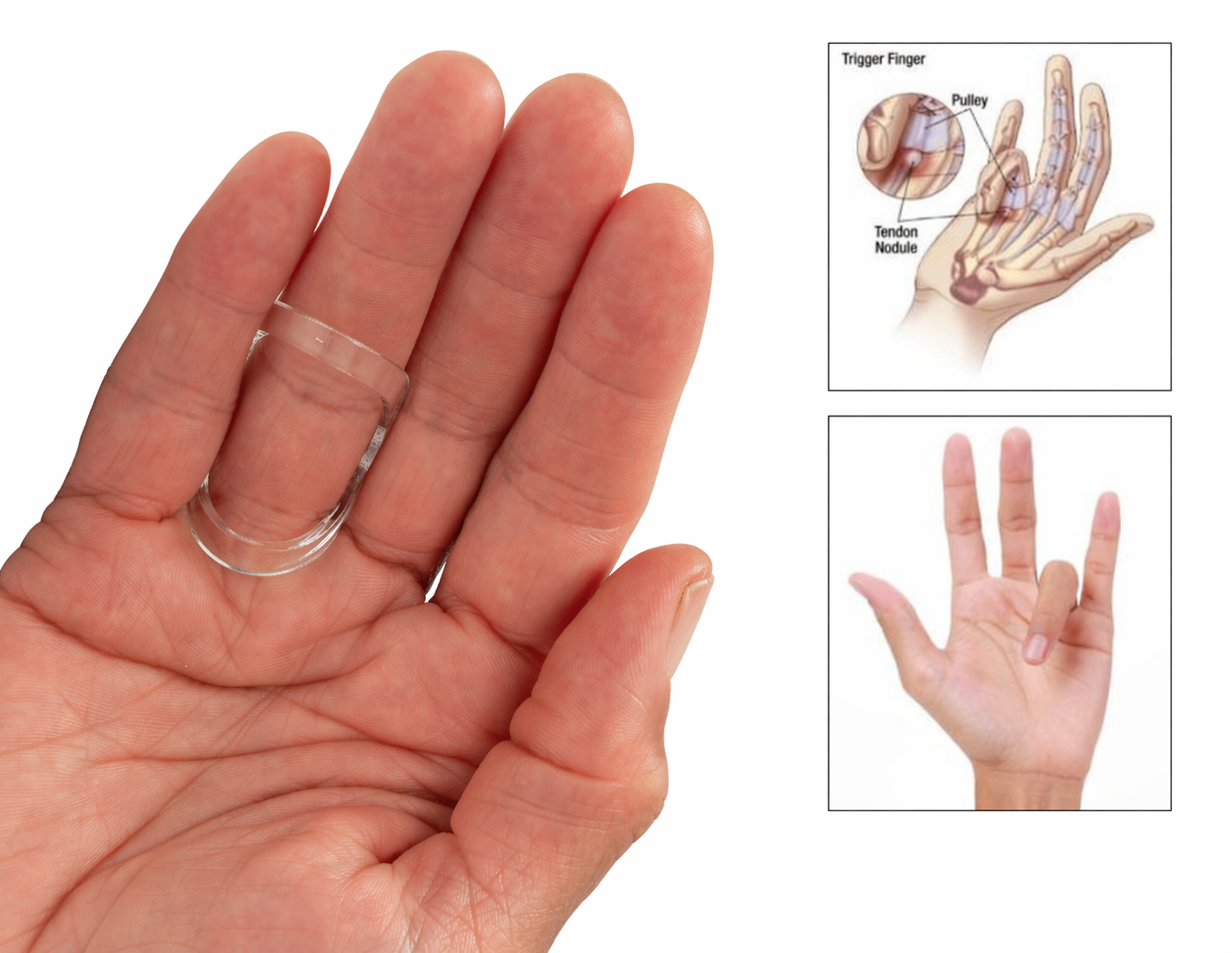
Trigger finger is a common condition encountered in clinical practice, characterized by finger locking, pain in the middle joint, and tenderness at the base of the finger. It most frequently affects individuals between the ages of 55 and 60 and has a higher prevalence in women. While surgery and injection are well-known for managing trigger finger symptoms, what about the use of splinting as an effective treatment option?
While corticosteroid injections and surgical release remain well-established treatment options, splinting is increasingly recognized as a valuable first-line, conservative intervention. This raises an important clinical question: What role does splinting play in effectively managing trigger finger?
|
Are you a Patient or Consumer?
|

Evidence for Splinting in Trigger Finger Management
A growing body of evidence supports splinting as an effective conservative treatment for trigger finger. Multiple studies have demonstrated meaningful reductions in pain and triggering with consistent splint use. Notably, one study reported that 87% of patients avoided surgery or corticosteroid injection at one-year follow-up after completing a splinting program. Additionally, a literature review found that combining splinting with corticosteroid injection may result in improved symptom resolution compared to either intervention alone.
Non-surgical management, including splinting, is typically recommended for mild to moderate cases, particularly when the digit can be actively extended without assistance. Standard protocols suggest continuous splint wear for approximately 6 weeks, with extension up to 10 weeks if symptoms persist. The splint may be removed periodically to perform tendon gliding exercises, which should be incorporated multiple times daily.
Recent research demonstrates symptom improvement with splinting at multiple joints, including the metacarpophalangeal (MCP), proximal interphalangeal (PIP), distal interphalangeal (DIP), and thumb interphalangeal (IP) joints. When selecting a splinting approach, clinicians should prioritize the position that promotes optimal tendon glide while minimizing functional restriction.
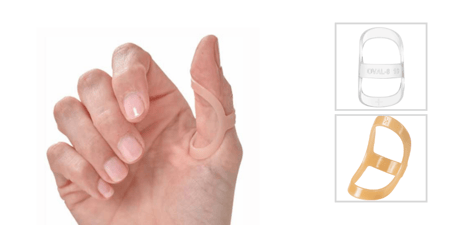
Splint Selection: The Role of the Oval-8® Finger Splint


The Oval-8® Finger Splint is a clinically versatile option for trigger finger/thumb management due to its:
- Low-profile, lightweight design for improved patient compliance
- Precise sizing options to ensure optimal fit
- Functional positioning of the PIP, DIP, or thumb IP joints
- Availability in Classic Beige and Clear for patient preference
Its design allows for targeted joint immobilization while preserving overall hand function—making it particularly suitable for patients who require continued daily hand use.
Key Takeaways for Clinical Practice
- Splinting is a validated, non-invasive first-line treatment for trigger finger
- Best outcomes occur in early-stage or flexible triggering cases
- Consistent wear and proper joint selection are critical to success
- Combining splinting with other treatments may further improve outcomes

Patients and Consumers
Are you looking for more information on Trigger Finger?